Case StudyMembers Only
IUS Monthly: Acute Severe Ulcerative Colitis
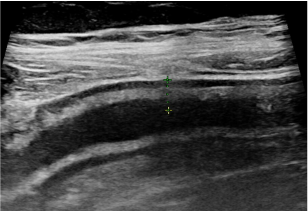
IUS Monthly case highlighting the role of intestinal ultrasound in monitoring acute severe ulcerative colitis.
July 8, 2025
IUS Monthly case highlighting the role of intestinal ultrasound in monitoring acute severe ulcerative colitis.